Can AI Build Trust in Indian Healthcare? Real-World Impact, Gaps, and Ethical Adoption

Advertisement

Artificial Intelligence has crossed the threshold from promise to presence in Indian healthcare. What was once discussed in conference halls and innovation summits is now embedded in radiology suites, pathology labs, teleconsultation platforms, hospital dashboards, and pharmaceutical research pipelines.
The conversation has shifted from “Will AI enter healthcare?” to “How fast is it scaling?” and, more importantly, “Can the system trust it?”
The answer will define the next decade of Indian healthcare.
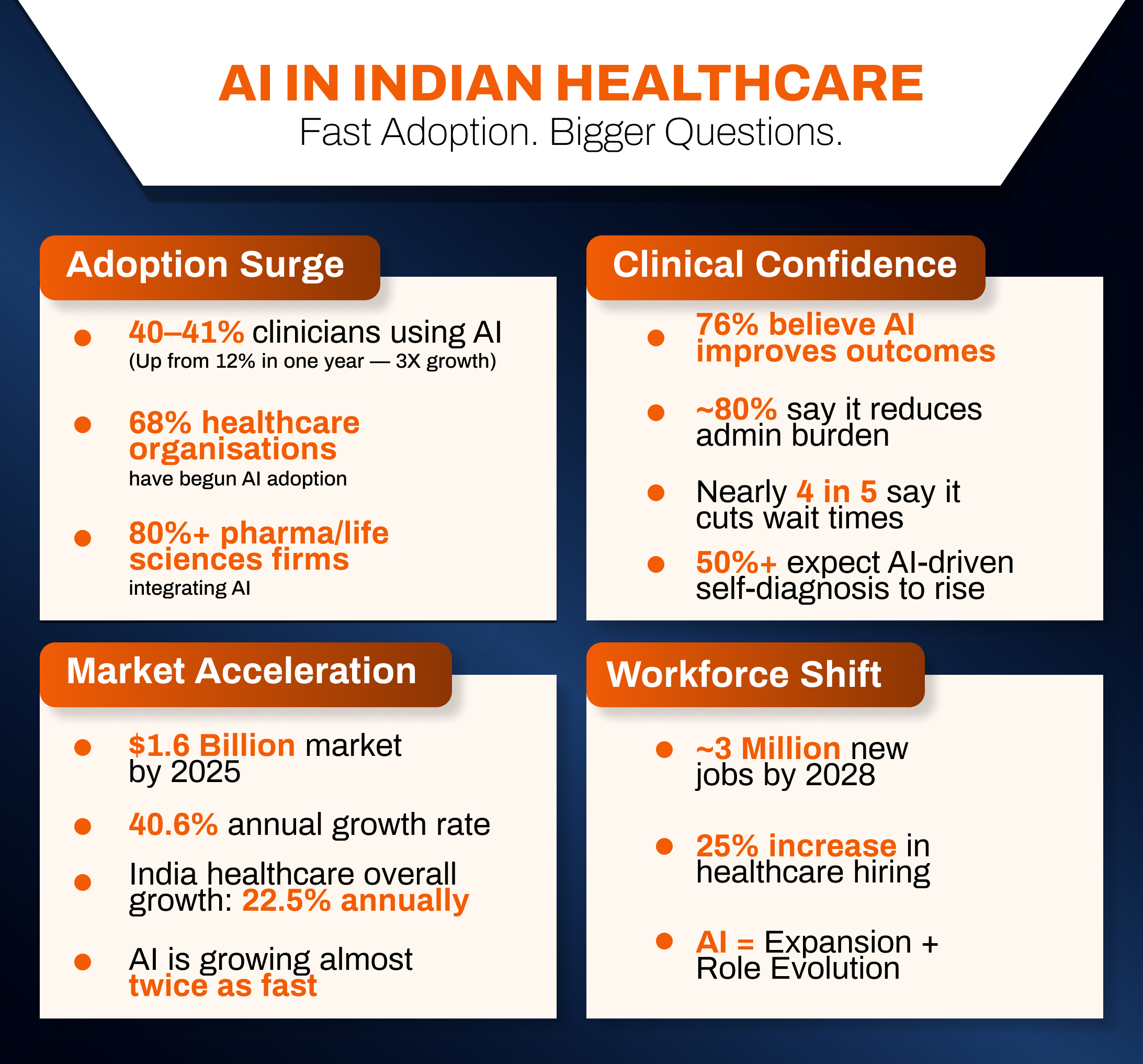
Today, nearly 40–41% of clinicians in India report actively using AI tools in their professional work, representing a more than threefold jump from approximately 12% just a year earlier. This is not incremental diffusion; it is acceleration. Adoption at this pace signals structural transformation rather than experimental enthusiasm.
Beyond usage, sentiment is equally telling. Around 76% of Indian healthcare professionals say they believe AI can improve patient outcomes. Close to four in five clinicians believe AI can reduce wait times. An even greater proportion sees automation as a pathway to reduce administrative overload. More than half anticipate that AI will soon empower patients to self-diagnose before clinical interaction.
The ecosystem is responding accordingly. Roughly 68% of healthcare organisations in India have initiated AI adoption, though many remain in pilot or proof-of-concept phases. In adjacent sectors such as pharmaceuticals and life sciences, adoption is even deeper, with over 80% of organisations integrating AI at some level into operations, analytics, or research.
The economic momentum is equally significant. The Indian AI healthcare market is projected to reach approximately $1.6 billion by 2025, expanding at an estimated 40.6% compound annual growth rate. To contextualise that growth, India’s broader healthcare sector itself expanded at roughly 22.5% annually between 2016 and 2022, driven by infrastructure expansion, digital health integration, and increased health spending.
AI is not riding healthcare’s growth wave. It is accelerating it.
And yet, for all its speed, scale, and statistical optimism, AI faces one defining test: trust.
The Structural Pressures Driving AI’s Rise
To understand why AI adoption is happening at such velocity, one must examine the structural constraints of Indian healthcare.
India’s population exceeds 1.4 billion. Disease burden is shifting from infectious diseases toward non-communicable illnesses, diabetes, cardiovascular disorders, cancer, and neurological conditions, which require long-term monitoring and early detection. Urban tertiary centers manage complex caseloads at volume, while rural districts face chronic shortages of specialists.
The doctor-patient ratio remains unevenly distributed. Radiologists, oncologists, neurologists, and pathologists are concentrated in metropolitan clusters. Diagnostic turnaround times can stretch. Administrative workloads overwhelm clinicians. Insurance documentation consumes clinical hours. Preventive screening remains inconsistent in semi-urban regions.
In such a system, AI does not enter as a novelty. It enters as a necessity.
Algorithms can process thousands of imaging scans in hours. Predictive systems can flag high-risk patients before deterioration. Digital triage can prioritise critical cases. Automated documentation tools can reduce clerical fatigue. Pattern-recognition engines can assist in identifying anomalies invisible to the human eye under time pressure.
For policymakers seeking scale, for hospital administrators seeking efficiency, and for clinicians seeking relief from cognitive overload, AI offers structural leverage.
But structural leverage does not automatically produce structural trust.
From Experimentation to Embedded Practice
The current phase of AI adoption in Indian healthcare can best be described as transitional. It is no longer confined to pilot programs, yet it is not fully institutionalised.
Nearly two-thirds of healthcare organisations have begun integrating AI tools. However, many remain in early-stage implementation. Proof-of-concept pilots are common. Full enterprise-wide integration remains less widespread. This suggests optimism, but also caution.
Pharmaceutical and life sciences sectors, by contrast, have moved faster. With over 80% incorporating AI in some capacity, drug discovery modelling, clinical trial optimisation, and supply chain analytics are rapidly becoming algorithmically enhanced. This divergence highlights a broader pattern: AI adoption progresses fastest where regulatory ambiguity is lower and risk accountability is clearer.
Clinical medicine, by nature, carries higher stakes.
Still, the rise in clinician usage from 12% to approximately 40% within a year is one of the strongest indicators that AI is crossing from peripheral assistance to embedded support. Such a dramatic increase implies not only the availability of tools but also perceived utility.
Clinicians are pragmatic adopters. Tools survive only if they deliver.
Diagnostics: The Frontline of AI Trust
If trust in AI is being built anywhere first, it is in diagnostics.
Radiology has become the flagship domain of AI integration. Image-recognition systems trained on vast datasets can detect nodules, lesions, and anomalies with consistency that reduces oversight errors. In tuberculosis screening programs, AI-assisted chest X-ray interpretation is being used to accelerate case identification. In oncology, mammography and pathology slide analysis are increasingly supported by algorithmic second reads.
Importantly, AI is not displacing clinicians. It is augmenting them.
Radiologists often describe AI as a “digital colleague”, one that does not tire, does not lose concentration after the hundredth scan, and can flag subtle deviations. The result is not replacement, but reinforcement.
Trust in this context emerges from repeatability. When an AI tool consistently flags the same anomaly that a trained specialist would identify, confidence grows. When it reduces reporting time without compromising accuracy, reliability is strengthened.
However, the inverse is also true. A single widely publicised error can undo months of gradual trust-building.
Telemedicine, Triage, and the Democratisation of Access
AI’s second major frontier lies in telehealth and remote monitoring.
As teleconsultation platforms expanded, AI tools began performing symptom pre-screening before patients even interact with physicians. These systems collect structured inputs, assess risk probability, and guide urgency. In chronic disease management, AI models analyse longitudinal data from glucose monitors, blood pressure devices, or wearable sensors, flagging patterns that may indicate complications.
This model is especially relevant in rural and semi-urban India, where specialist access remains limited. AI-supported triage allows general practitioners or frontline health workers to escalate cases appropriately.
More than half of clinicians now anticipate that patients will increasingly use AI systems to self-assess symptoms before visiting clinics. This shift represents a fundamental transformation in patient agency. Healthcare may move from reactive to proactive engagement.
But it also introduces new vulnerabilities.
Self-diagnosis powered by AI could reduce unnecessary visits. It could also generate anxiety, misinterpretation, or overreliance. Trust, in this context, must be accompanied by literacy.
Economic Stakes: Growth, Jobs, and Systemic Realignment
The projected expansion of the AI healthcare market to $1.6 billion by 2025 reflects not just technology sales, but ecosystem transformation.
With an estimated 40.6% annual growth rate, AI in healthcare is expanding nearly twice as fast as the broader healthcare sector itself. Venture capital flows, startup ecosystems, public-private partnerships, and hospital procurement strategies are aligning around algorithmic solutions.
Perhaps most consequentially, AI adoption is expected to generate nearly 3 million new jobs in healthcare by 2028. Contrary to simplistic automation fears, digital transformation appears likely to reconfigure rather than eliminate workforce roles.
Data scientists, AI validation specialists, health informatics professionals, digital ethicists, and implementation engineers will become embedded within hospital systems. Meanwhile, overall healthcare hiring could increase by approximately 25% by 2028, driven by digital transformation needs.
The workforce will not shrink. It will evolve.
Yet workforce evolution introduces its own trust equation. Clinicians must trust AI outputs. AI engineers must understand clinical nuance. Administrators must align incentives with patient outcomes rather than technological novelty.
The Trust Deficit: What Could Go Wrong?
Despite enthusiasm, three fault lines threaten AI’s trust trajectory: opacity, bias, and accountability.
Opacity
Many advanced AI systems operate as “black boxes,” generating outputs without intuitive explanation. Clinicians trained in evidence-based reasoning may hesitate to rely on recommendations whose internal logic they cannot interrogate.
Trust in medicine is grounded in justification. If AI cannot provide interpretable reasoning pathways, clinicians may treat it as advisory rather than authoritative.
Bias
AI models are only as representative as the data on which they are trained. If datasets are disproportionately urban, male, or economically homogeneous, algorithmic outputs may perform suboptimally across diverse populations.
In a country as demographically complex as India, bias is not theoretical; it is systemic risk.
Accountability
If an AI-assisted decision contributes to an adverse outcome, who bears responsibility? The software developer? The hospital? The clinician? Legal clarity remains emergent rather than settled.
Without clear accountability frameworks, institutions may hesitate to deploy AI at scale.
Governance as the Deciding Variable
If AI’s trajectory in Indian healthcare hinges on trust, governance becomes the central variable.
India has begun constructing data protection and digital health frameworks. Yet AI-specific clinical governance requires deeper standardisation.
Validation protocols must be transparent. Model performance across demographic subgroups must be publicly documented. Certification pathways should distinguish between decision-support tools and autonomous systems. Continuous post-deployment monitoring must be mandatory rather than optional.
Trust cannot rely on marketing claims. It must rest on measurable accountability.
A 2030 Scenario: Two Possible Futures
By 2030, India could emerge as a global leader in ethical, large-scale AI healthcare deployment. With its digital public infrastructure, strong IT ecosystem, and expanding health technology market, the foundations exist.
In one scenario, AI becomes seamlessly integrated, validated across diverse populations, explainable to clinicians, secure in its data architecture, and governed by clear regulatory standards. Patients experience shorter wait times, earlier diagnoses, and personalised care. Clinicians experience reduced burnout. Public health systems anticipate outbreaks rather than react to them.
In another scenario, fragmented pilots remain unstandardised. Bias incidents erode public trust. Legal ambiguity slows adoption. AI becomes viewed as an efficiency tool rather than a care partner.
The difference between these futures will not be algorithmic sophistication. It will be trust architecture.
Trust Is the Infrastructure
Adoption rates of 40%. Professional optimism of 76%. Market growth toward $1.6 billion. Millions of projected new jobs. Sixty-eight percent organisational uptake. Eighty percent pharma integration.
The numbers indicate momentum.
But healthcare is not an industry that tolerates unexamined acceleration. It demands ethical coherence.
Trust in AI will not be built through press releases or pilot announcements. It will be built through consistent validation, transparent communication, clinician education, inclusive data practices, and regulatory clarity.
AI has entered Indian healthcare decisively. Whether it remains an assistant, becomes a partner, or evolves into an indispensable infrastructure will depend on how seriously trust is engineered.
Technology scales rapidly. Trust scales slowly.
India now stands at the intersection of both.
And the choices made in this decade will determine whether AI becomes healthcare’s most reliable ally, or its most contested innovation.
Stay tuned for more such updates on Digital Health News